
Imagine losing your sight, then being offered it back through brain surgery. Not a new eye. Not a transplant. A chip that writes light directly into your mind. That is the promise behind the Neuralink Blindsight human trials, and it forces a strange question: if a machine draws the picture and your brain reads it, are you really seeing again, or learning a new sense from scratch?
For the underlying science, see our explainer on how brain-computer interfaces actually read your thoughts.
The technology is real, and it is close. Musk has said Neuralink is “ready” for its first human Blindsight implant, awaiting final regulatory sign-off (MobiHealthNews). But “ready” and “restores vision” are not the same claim. What blind volunteers can actually expect sits somewhere between a genuine breakthrough and a hard scientific ceiling that no amount of engineering hype can lift.
Let’s separate the two.
What the Blindsight visual cortex implant actually does
Most vision aids work with the eye. Blindsight ignores it.
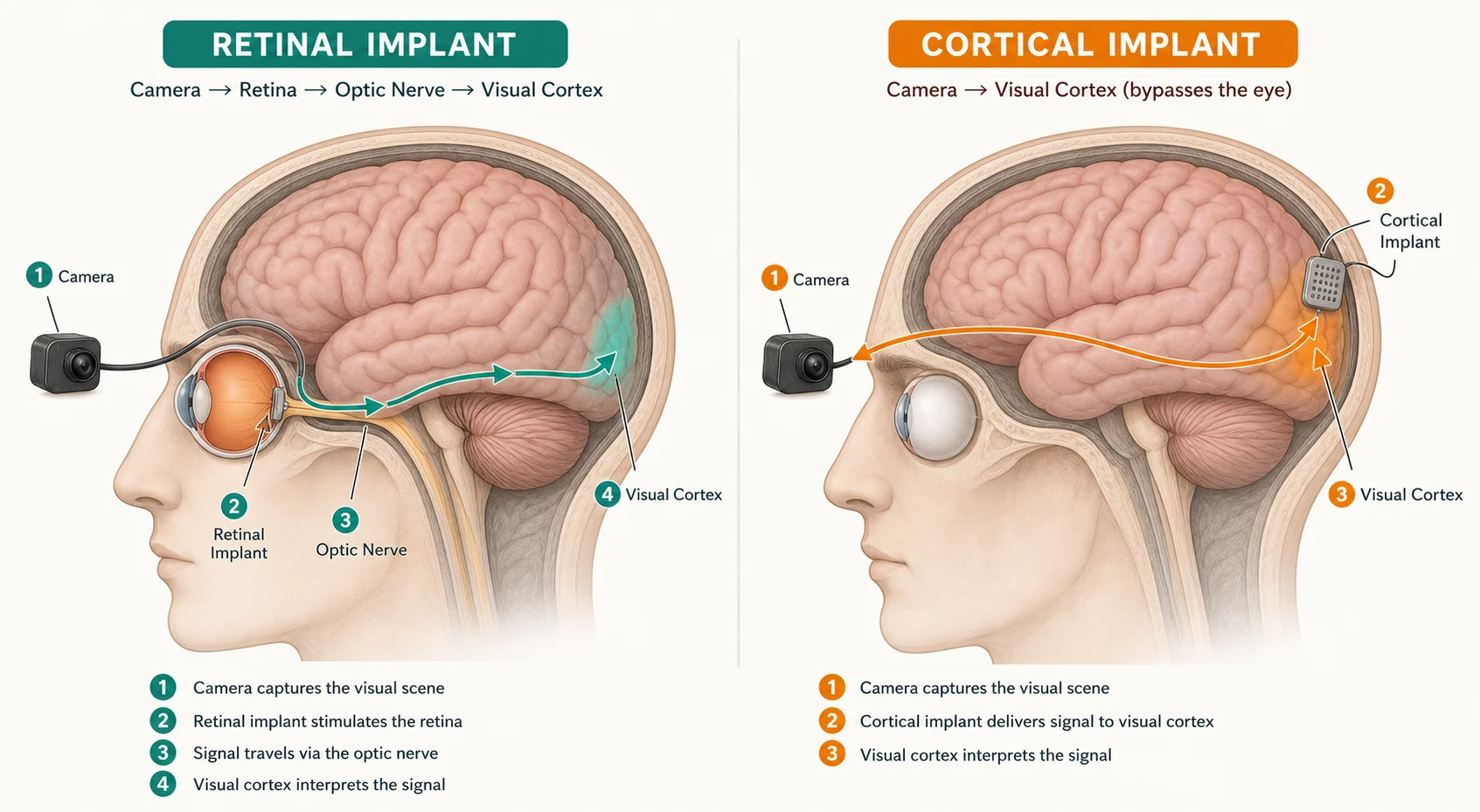
The device places a microelectrode array directly into the visual cortex, the patch of tissue at the back of the brain that turns nerve signals into the experience of seeing. It bypasses damaged eyes and optic nerves entirely and activates cortical neurons itself (PIE Magazine). A camera feeds the system, and the implant translates that feed into patterns of stimulation.
Early hardware is dense. Neuralink’s array uses 96 flexible threads carrying 32 electrodes each, so 3,072 electrodes in total (Wikipedia). That number gets quoted a lot, usually to imply high-definition sight. Hold that thought, because the electrode count is exactly where the story gets complicated.
The upside of skipping the eye is huge for eligibility. Because it targets the cortex, Blindsight could in principle help people with no functioning eyes at all, and possibly those blind from birth, as long as the visual cortex itself is intact and confirmed by MRI (Teslarati).
How does Neuralink Blindsight work at the level of a single dot of light
Here is the mechanism, minus the mystique.
The visual cortex is organized retinotopically. That means a specific spot on the cortex corresponds to a specific point in your field of view. Stimulate a neuron there and the person perceives a phosphene, a small bright dot at the matching location (neurapod). Fire many electrodes in a deliberate pattern and, in theory, those dots assemble into shapes, letters, and eventually crude images.
Think of it like a stadium crowd holding up cards to spell a word. Each card is one phosphene. The message only works if every card lights at the right moment in the right seat.
Now the catch. A screen’s pixels are uniform and independent. Cortical neurons are not. A 2024 technical analysis found that even a 45,000-electrode simulation produced a blurry result far worse than a 45,000-pixel image, because stimulating one neuron creates a blob about the visual size of “a pinkie held at arm’s length,” and a single point of real light can activate thousands of overlapping neurons (The Conversation).
That is the receptive-field problem, and it is the single most underreported fact in this whole story. More electrodes do not translate cleanly into sharper vision. As one team put it, “even a single star, a single bright pixel, generates an immensely complex neural response in the visual cortex.” Neuralink’s own writing-into-the-brain challenge echoes the tension we explored in the ethics of writing signals into the brain: controlling what the brain perceives is far messier than flipping pixels on a display.
From primate trials to FDA Breakthrough Device Designation
The animal data is encouraging, and worth reading carefully.
In non-human primate trials, blind monkeys directed their gaze toward visual stimuli in at least two-thirds of attempts, which fits with induced visual percepts (neurapod). Neuralink engineer Joseph O’Doherty reported similar results in mid-2025, with stimulation triggering gaze shifts toward virtual targets (tesorb). A monkey looking the right way is a real signal. It is not a monkey reading an eye chart.
On the regulatory side, the FDA granted Blindsight Breakthrough Device Designation on September 18, 2024 (Neuralink). That sounds like an endorsement. It isn’t approval. The designation only speeds up review and gives the company closer contact with FDA reviewers during the premarket process (Medical Device Network). The green light for a first implant still hasn’t come publicly.
Context helps. Neuralink has already implanted its separate Link device, built for movement and speech rather than vision, in five patients, and it opened a global patient registry in April 2025 (Teslarati). So the company has surgical experience with brain implants. Vision is a different and harder target.
What the first Neuralink Blindsight human trials participants can expect
Set the marketing aside and the expectations get modest, fast.
Neuralink has said so itself: initial vision will be low-resolution, comparable to early video-game graphics, the “Atari-level” description that keeps circulating (PIE Magazine). Independent experts push harder. IEEE Spectrum’s reporting concludes Blindsight will almost certainly disappoint against Musk’s public claims, noting that no company has yet commercialized a cortical visual prosthetic at all (IEEE Spectrum).
History backs the caution. The comparable Orion cortical prosthesis produces basic shapes and light patterns rather than photographic detail, even now (Ophthalmology Times Europe). Vision scientist Gislin Dagnelie of Johns Hopkins has also flagged how little Neuralink has actually disclosed: “I’m leery about the fact that they are very superficial in their description of the devices.”
So what would success look like for an early volunteer? Realistically, this:
- Perceiving light versus dark, and rough motion
- Locating a doorway, a face-shaped blob, or a bright object
- Slowly learning to interpret phosphene patterns over months
- Not reading text, recognizing faces, or seeing color at first
And the risks are not trivial. This is open surgery near the visual cortex. It carries the standard neurosurgical dangers of infection, bleeding, and seizures, plus device failure and the very real chance that the payoff falls short of the hope that drove someone to volunteer.
Musk has floated the idea that Blindsight might one day exceed natural vision, adding infrared or radar wavelengths “like Geordi La Forge.” Maybe someday. The gap between that pitch and Atari-level dots is the honest headline.
Who qualifies, and the access question nobody wants to ask
No official inclusion criteria for Blindsight exist yet, as of early 2026.
Based on Neuralink’s other trials, the expected profile is a profoundly blind adult, roughly 22 to 75, with an intact visual cortex confirmed by MRI, a stable caregiver, and the stamina for extended follow-up, while excluding major psychiatric conditions or surgical risk factors (medpath trial tracking). Interest is already outrunning enrollment: a blind Korean YouTuber publicly volunteered for the trial in March 2026 (The Korea Times).
Here is the tension I keep coming back to. Cortical implants are, on paper, more inclusive than retinal ones. Argus II needed a working optic nerve and retina, which ruled out huge numbers of blind people (PMC). Blindsight, by stimulating the cortex directly, could reach people retinal implants never could (PMC review).
More inclusive in principle. Then look at the rollout. The planned first human site is a UAE-PRIME study through a Cleveland Clinic Abu Dhabi partnership. One company, one expensive novel neurosurgery, gatekeeping who sees first. That is the same worry we raised in will brain chips deepen the human class divide?: a technology that could level a disability may still arrive along the usual lines of wealth and geography. And once a device can write vision into the brain, the questions about consent and data raised in neuroprivacy stop being abstract.
What to watch for next
Skip the hype cycle and track a few concrete signals instead. Watch for actual FDA clearance rather than another designation. Watch for the first implant to happen at all, and for independent researchers, not company posts, to describe what the patient can do. Watch whether early users read letters or only sense light.
I want this to work. A device that gives a congenitally blind person any spatial sense of the world would be genuinely historic, and the cortical approach is the most inclusive route we have. But wanting it to work is not the same as pretending the receptive-field ceiling isn’t there.
The most useful thing you can do as a reader is hold both truths at once. Real progress. Real limits. If you follow neural interfaces, the framework for judging what comes next is in cognitive enhancement ethics — because the line between restoring a sense and augmenting one is exactly where this story goes next. So when the first patient wakes up with a chip reading light into their brain, ask not just whether they can see, but what kind of seeing we decided was good enough to call a cure.