Ask the wrong question and you get a leaderboard. Ask “who has the most electrodes?” and Neuralink and Paradromics win, Synchron loses, end of story. But that’s not the choice a paralyzed patient actually faces.
The real question in the Neuralink vs Synchron vs Paradromics debate is quieter and much harder. Which risk would you accept, for which capability, and who is each device actually built for? These three companies have split into two rival philosophies about how a machine should reach into a human brain. One bets on raw bandwidth. One bets on staying out of the operating room. And the “winner” changes depending on whose brain we’re talking about.
So let’s compare them the way a patient would — not the way a spec sheet would.
Two philosophies, three companies
Strip away the branding and there are really only two ways into the brain.
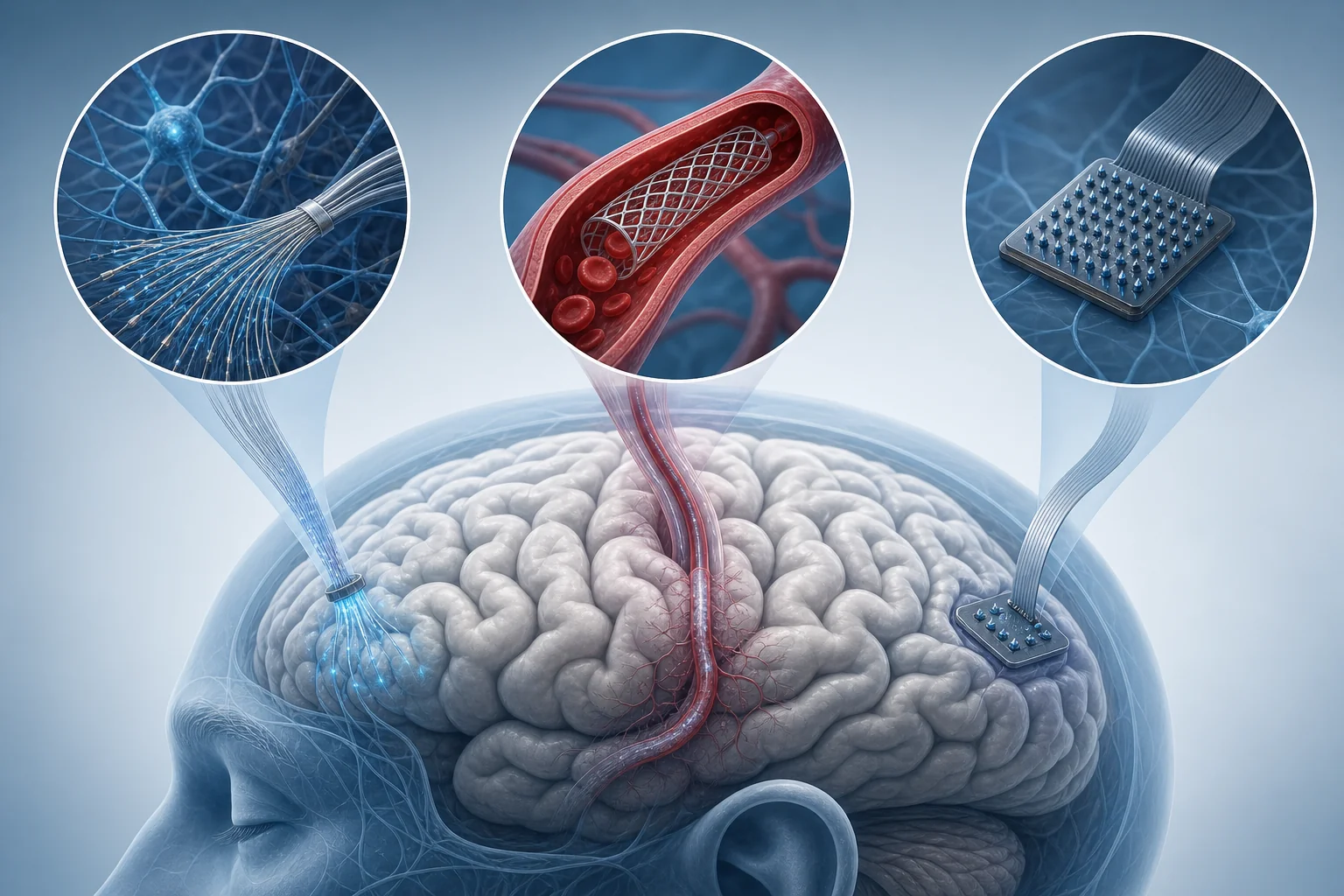
The first is intracortical: you push tiny electrodes directly into brain tissue. You get a strong, high-resolution signal and a lot of it. The cost is open-brain surgery. Neuralink and Paradromics both take this route (Auctores comparative review, 2025).
The second is endovascular: you thread a device through a blood vessel and park it near the brain, no craniotomy required. The signal is weaker and coarser. Synchron owns this lane.
That single fork — deeper for a richer signal, or shallower for a safer one — explains almost every difference that follows. As Rice University bioengineer Jacob Robinson frames the trade-off, deeper and more invasive electrode placement yields richer data but carries greater surgical risk.
Neuralink: maximum bandwidth, maximum access
Neuralink’s N1 implant is the maximalist bet. It uses 64 ultra-flexible polymer threads, each carrying 16 platinum-iridium electrodes, for 1,024 total recording channels. A surgical robot stitches those threads directly into the cortex.
Does it work? So far, yes. Neuralink’s PRIME trial grew from 12 to 21 participants over 2024 and 2025, with zero serious device-related adverse events reported. Participants have hit typing speeds of up to 40 words per minute. By summer 2025, cursor-control speeds reached roughly 8 bits per second — right in the range of an able-bodied person using a mouse.
That last number matters more than the electrode count. Matching a healthy mouse user is the threshold where a brain implant stops being a demo and starts being genuinely useful.
Paradromics: the bandwidth bet, a different route in
Paradromics is chasing the same prize as Neuralink — the highest possible data rate — but with different hardware. Its Connexus array packs more than 1,600 penetrating microelectrodes onto a monolithic silicon chip, sampling at 30 kHz per channel (Auctores, 2025).
On paper, that’s the most aggressive data pipeline of the three. The catch is the phrase “on paper.” Paradromics only performed its first chronic human implant in 2026, after receiving an FDA Investigational Device Exemption in November 2025 for its Connect-One study. Surgeons at the University of Michigan placed a 421-microelectrode version of the wireless Connexus in a patient who had lost speech, aiming to restore communication for people with ALS and related conditions.

Robinson put the situation plainly: Paradromics “has the highest-bandwidth interface, but they haven’t demonstrated it in humans yet” (MIT Technology Review). Potential and proof are not the same thing.
Synchron: betting on safety and scale
Synchron went the other way entirely. Its Stentrode carries just 16 electrodes — a rounding error next to Neuralink’s 1,024. They sit on a nitinol stent scaffold, delivered up through the jugular vein. No open skull. No robot stitching threads into your cortex.
Fewer electrodes means a coarser signal. But look at what that buys. Synchron’s six-patient COMMAND study met its primary safety endpoint at 12 months with no serious adverse events and stable performance. The company has now implanted its device in 10 human patients.
Synchron also leads on paperwork, which turns out to matter enormously. It received FDA Breakthrough Device Designation back in August 2020 and holds the first-ever IDE for a chronically implanted BCI. In November 2025 it raised a $200 million Series D to fund a 2026 pivotal trial — and what it expects to be the first-ever PMA filing for an implanted brain-computer interface (The Robotics Media).
There’s a philosophical trade here too. Synchron’s read-focused device reads intent; it doesn’t write signals back into the brain. That “read-only” limit dodges a thornier ethical frontier — the questions raised by writing signals into the brain, which higher-bandwidth systems eventually invite.
Neuralink vs Synchron vs Paradromics: the numbers that actually differ
Here’s the whole comparison in one place — the table nobody covering this trio has put together cleanly.
| Dimension | Neuralink (N1) | Paradromics (Connexus) | Synchron (Stentrode) |
|---|---|---|---|
| Approach | Intracortical, penetrating | Intracortical, penetrating | Endovascular, minimally invasive |
| Electrodes / channels | 1,024 across 64 threads | 1,600+ microelectrodes | 16 |
| Surgery | Open-brain, robot-implanted | Open-brain | No craniotomy; via jugular vein |
| Human progress | 21 PRIME participants | First chronic implant in 2026 | 10 patients implanted |
| Demonstrated performance | ~8 bps; up to 40 WPM typing | Highest bandwidth on paper, unproven in humans | Stable, safety-endpoint met |
| Regulatory status | FDA Breakthrough Device | FDA Breakthrough Device; IDE Nov 2025 | Breakthrough Device (2020); first BCI IDE; PMA filing planned 2026 |
Read the table sideways and the pattern jumps out. No single column wins every row. High bandwidth and human proof sit in different companies.
Who is each approach actually for?
Specs don’t get implanted. People do. So match the device to the person.
- Synchron fits the risk-averse. A patient who can’t survive — or won’t accept — a craniotomy has a real option here. Lower ceiling on capability, much lower surgical risk.
- Neuralink fits the proven-capability seeker. For someone who wants demonstrated, mouse-grade control today, PRIME’s track record is the strongest evidence going.
- Paradromics fits the maximum-bandwidth case. An ALS patient who has lost speech and needs the richest possible signal to communicate is exactly who Connexus is built for — once the human data catches up to the promise.
This is also where the ethics stop being abstract. If the highest-bandwidth implants stay expensive and surgical, access won’t be evenly distributed — the same worry behind whether brain chips could deepen the human class divide. And the more a device reads, the sharper the questions get about what that neural data reveals and who can demand it.
The regulatory pathway problem
Here’s the twist that raw performance hides. Being safer or further along in trials doesn’t mean you reach patients first. The FDA route decides that.
Synchron is aiming for a PMA — Premarket Approval — the most rigorous, slowest pathway the FDA has. That’s a signal of confidence, but it’s also a longer road than the Breakthrough or De Novo routes. Neuralink and Paradromics also hold Breakthrough Device status, yet they’re earlier in enrollment scale.
So “furthest along” has no clean answer. Measure it by patient-years, and Synchron leads. Measure it by participant count, and Neuralink pulls ahead. Measure it by demonstrated bandwidth potential, and Paradromics tops the chart. Three different yardsticks, three different frontrunners.
If you’ve followed our look at the competing “vs” architectures in AI, the shape is familiar: no universal best, just the right tool for a specific job.
So which one should we trust?
I won’t crown a winner, because the honest answer refuses one.
Trust Synchron if you’d rather keep your skull intact and accept a modest signal. Trust Neuralink if you want the most human proof behind a high-bandwidth implant right now. Trust Paradromics if your need is bandwidth above all and you can wait for the data to arrive.
What’s actually striking is that the field hasn’t collapsed into one design. That’s a good sign. A brain is not a phone — there’s no reason a single form factor should suit every patient, every condition, every tolerance for risk. The interesting future isn’t one company winning. It’s these three philosophies coexisting, each owning the patients it serves best.
Which risk would you accept, for which capability? Sit with that question. It’s the one that actually matters — and the one no spec sheet will answer for you.