
You lie still inside the scanner. A technician says you’ll get results in a few days. What nobody mentions is that the first look at your images might not come from a doctor at all. It might come from a model. That quiet handoff has a name now, and in 2026 it sits at the top of medicine’s worry list: the AI diagnostic dilemma.
It’s no longer a niche worry. The patient-safety nonprofit ECRI named “navigating the AI diagnostic dilemma” the number one item on its annual list of top patient-safety concerns, warning that overreliance on these tools can quietly feed diagnostic errors (TechTarget).
Here’s the question worth sitting with. When a machine reads your scan, who is actually deciding your diagnosis? The honest answer is messier than “the AI” or “the doctor.” It’s both, and the seam between them is exactly where things go wrong.
What ECRI actually flagged as the top patient-safety concern
ECRI didn’t say AI is bad. It said the way hospitals lean on AI is risky.
The organization ranked the diagnostic dilemma above reduced rural healthcare access, rising preventable disease, and federal funding cuts (Becker’s Hospital Review). That’s a striking placement. It puts a software problem ahead of some very concrete, physical gaps in care.
Why so high? Because oversight of that first automated read is inconsistent across health systems. The standard advice from the report is that AI should “supplement, not replace” clinical judgment. Sensible on paper. The trouble is that the research on how humans actually behave around these tools tells a different story.
Two ways AI gets your diagnosis wrong
There are two failure modes worth understanding, and they pull in opposite directions. One is the model failing. The other is the human trusting it too much.
The model that works everywhere except your hospital
An AI that dazzles in testing can quietly fall apart once it leaves home.
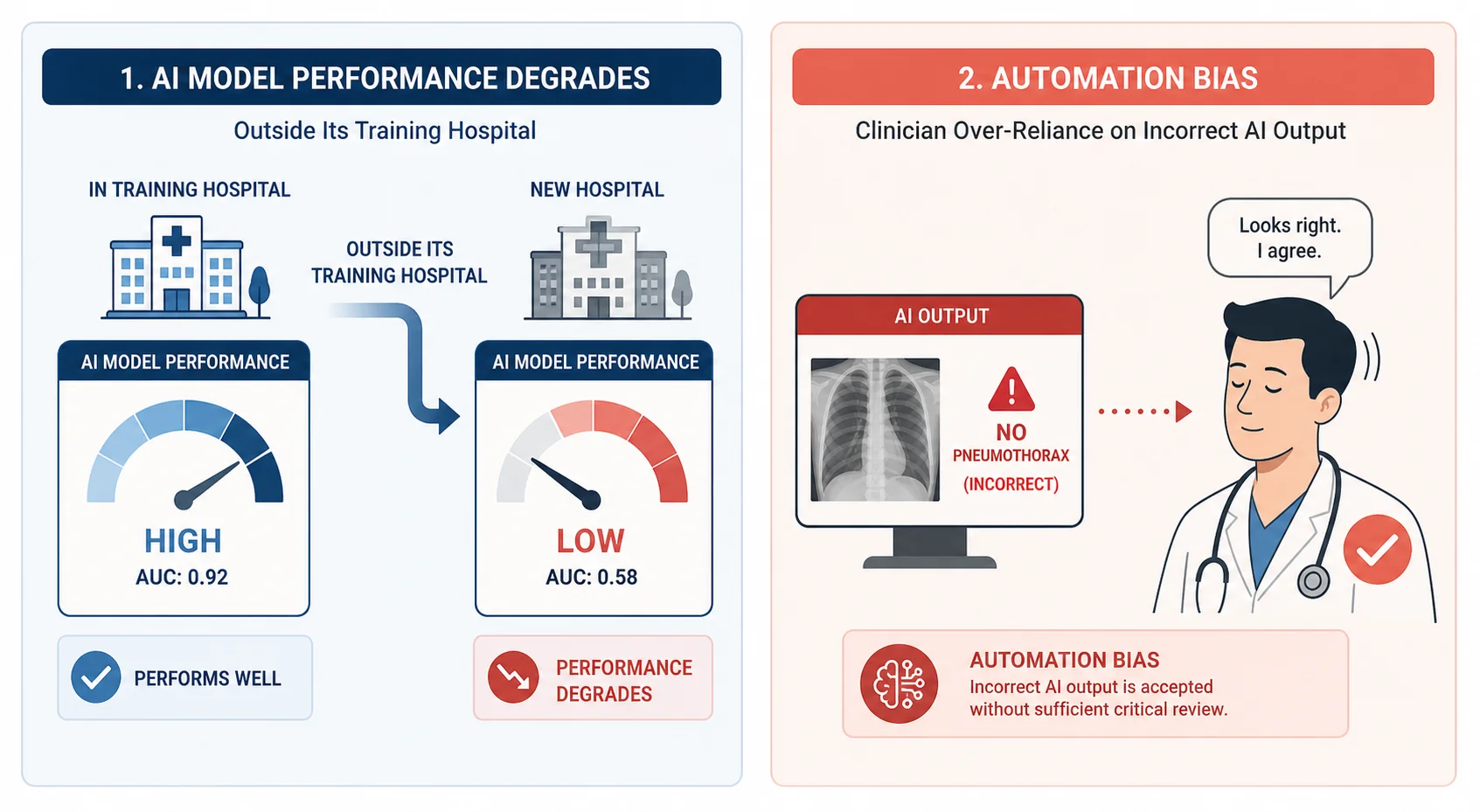
A 2026 systematic review found that radiology models lost up to 24% of their specificity when deployed outside the hospital that trained them (PMC). Specificity is the model’s ability to correctly rule out disease. Lose a chunk of it and you get more false alarms, more follow-up scans, more anxiety.
The cause has a dry name: distributional shift. In plain terms, the model learned your scanner’s quirks instead of the disease. It memorized how one hospital’s machines calibrate light and contrast, not what a tumor actually looks like. Move it down the road to a different scanner and its confidence no longer matches reality.
The clinician who defers to a wrong machine
Now flip it. Say the AI is wrong on your case. Will the human catch it?
Often, no. In a randomized study of 40 clinicians reading knee MRIs, AI assistance pushed diagnostic accuracy from 87.2% up to 96.4% (ESMO Real World Data and Digital Oncology00012-3/fulltext)). A real gain. But dig into the errors that remained, and 45.5% of them traced back to automation bias, clinicians deferring to an incorrect AI call rather than trusting their own read.
The same body of research found that when the AI gave a wrong recommendation, radiologists’ error rates climbed 12 to 15%, even among experienced readers. ECRI’s 2026 report put the psychology bluntly: when the system highlights a lesion, the human clinician is psychologically primed to agree with the machine.
Read that back. The tool meant to catch human error can manufacture a new one, by making the human stop looking.
The deskilling problem: what happens to human judgment
There’s a slower danger underneath all this. Use the tool long enough and the human skill it was supposed to back up starts to fade.
We already have a real-world signal. In a multicentre study across four endoscopy centres, experienced doctors, each with more than 2,000 prior colonoscopies, saw their adenoma detection rate fall from 28.4% to 22.4% in their non-AI procedures after regular exposure to an AI polyp-detection tool (STAT News). That’s a six-point drop in cases the AI wasn’t even involved in. Researchers called it the first documented real-world clinical deskilling effect.
Think about what that means. The tool didn’t just help on the day. It reshaped how the doctor sees, even when the tool was switched off.
Deskilling isn’t only about manual technique. Reviews describe it across several layers: the erosion of hands-on skill, of reasoning, even of the sensitivity that lets a clinician notice something feels off before they can name it. It’s the same tension we’ve traced in cognitive enhancement ethics, where offloading a mental task to a machine quietly changes the person doing the offloading.
Whose diagnoses AI gets wrong more often
Not everyone carries this risk equally. And medicine has been here before AI ever arrived.
Consider the pulse oximeter, the little clip on your finger. For decades it has overestimated blood oxygen in patients with darker skin, because melanin interferes with its light-based reading and the devices were calibrated on too few dark-skinned patients (Johns Hopkins Bloomberg School of Public Health). The result was delayed treatment for people whose real oxygen levels were dangerously low. Regulators still don’t require diverse-population testing.
That’s the pattern AI inherits, at scale. ECRI’s own framing is that models are only as reliable as their training data, and unexamined algorithms risk perpetuating biases that worsen health disparities. A scan-reading model trained mostly on one population can be quietly worse for everyone outside it, and nobody in the room may know. It’s the medical version of the divide we explored in will brain chips deepen the human class divide: a technology’s benefits and its blind spots rarely land on the same people.
Do patients actually trust AI over their doctor?
You might assume people reject the idea of a machine diagnosing them. The data says it’s closer than that.
In a blinded, NIH-funded survey of 2,472 diverse participants, more than 52% chose a human doctor while roughly 47% chose an AI method (University of Arizona Health Sciences). A near-even split. Machines have already earned a lot of trust.
Two details make that number more interesting. First, trust isn’t fixed. When participants were told their own physician considered AI a helpful adjunct, their acceptance of it went up on re-questioning. Your doctor’s endorsement moves the needle more than the technology itself does.
Second, the picture may be shifting. Newer 2026 survey coverage suggests public trust in healthcare AI is slipping rather than settling (Medical Xpress). The split could be widening away from AI, not toward it.
The AI diagnostic dilemma: what “a tool, not a replacement” really means
Here’s the sharpest thread, and the one the news coverage keeps skipping.
Legally, the human never left the hook. Under current malpractice law there’s no doctrine that moves liability from the treating physician to an AI tool or its maker. The doctor is judged against the reasonable-physician standard whether or not AI was used (Johns Hopkins Carey Business School). Hospitals can be liable for botched vetting or training. Device makers can face product claims if the tool itself fails. But the person accountable for your diagnosis is still a person.
Sit that next to the automation-bias data and the contradiction jumps out. The law says the human is fully responsible. The evidence says the human is primed to defer to the machine anyway. That gap, between who is accountable and who is actually deciding, is the real AI diagnostic dilemma. “Supplement, not replace” is a hope about behavior, not a description of it.
This isn’t a new kind of problem for anyone who follows how we govern powerful systems. We’ve watched the same lag between capability and rules play out in AGI regulation, where the technology sprints and the accountability framework limps behind.
Where this leaves you, the person in the scanner
So, back to the scanner. Should you be scared? No. Should you be a little more curious about what happens after the images leave the room? I think so.
Ask whether a clinician independently reviewed your scan or mostly signed off on the model’s read. Ask what the tool was validated on. These aren’t hostile questions. They’re the questions that keep a human genuinely in the loop instead of nominally on the form.
The uncomfortable truth is that the machine and the doctor are now reading together, and neither is fully in charge. Getting that partnership right is one of the defining problems of AI in medicine this decade. Until it’s settled, the smartest thing a patient can do is stay awake to the question the scanner never asks out loud: who’s really reading this?