
If you care for someone with paralysis, work in rehab, or follow medical technology closely, the main question is no longer whether neural implants can do anything useful. They can. The harder question is what they can restore right now, for whom, and under what conditions. That is where the conversation needs more precision.
In 2026, neural implants for paralysis are producing real gains in selected patients. Some systems help reconnect brain intention to spinal stimulation so a person can stand or step. Others help people with severe paralysis control a computer or assistive device without open-brain surgery. That is real progress. It is not a universal cure, and it is still far from routine care.
Why 2026 feels different
For years, paralysis technology lived in two separate worlds. One was the world of inspiring lab videos and proof-of-concept demos. The other was the world of everyday clinical reality, where most people still had to rely on wheelchairs, physical therapy, caregiver support, and assistive devices that did not restore lost motor pathways.
That gap has not disappeared, but it has narrowed.
What makes 2026 feel different is that movement restoration is no longer only an abstract promise. Researchers have already shown that a fully implanted brain-spine interface can reconnect cortical signals to spinal stimulation in a person with chronic spinal cord injury, allowing standing, walking, and more fluid transitions between movements. Earlier work on targeted epidural neuromodulation also showed that carefully timed spinal stimulation paired with rehabilitation can restore meaningful voluntary control in people with spinal cord injury.
At the same time, brain-computer interfaces are becoming more clinically mature. The point is not only dramatic movement recovery. For some people, the first major restoration is control over communication, digital tools, or external assistive systems. That may sound less dramatic than walking, but for people with severe paralysis, that kind of regained agency can be life-changing.
There is also a regulatory signal that matters. On March 16, 2026, Nature reported that China approved a brain implant for severe paralysis to help restore hand movement through a soft robotic glove, describing it as a world first for this kind of paralysis-focused BCI approval. That does not mean the field is solved. It does mean the conversation has moved beyond speculation.
The right way to read 2026 is this: we are now looking at repeatable categories of restoration, not isolated science fiction moments. But those categories are still narrow, selective, and heavily dependent on rehab, engineering support, and patient fit.
The three main ways these systems restore function
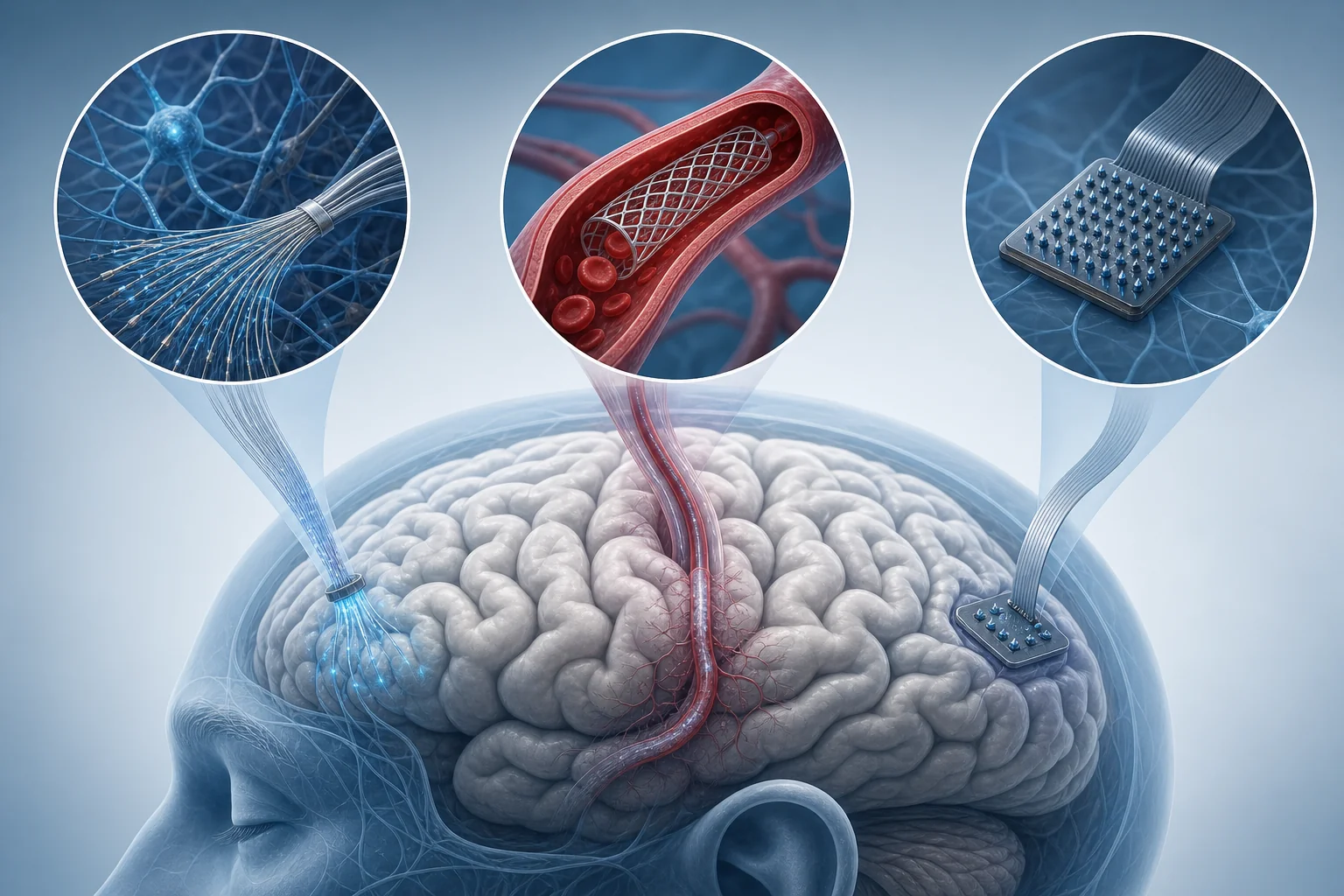
One reason the public gets confused is that “neural implant” gets used as if it describes one treatment. It does not. There are at least three very different paths here.
1. Brain-spine interfaces
These systems try to bridge the injury itself. Signals linked to movement intention are recorded from the brain, decoded by software, and translated into stimulation commands for the spinal cord below the injury. The goal is not just to move a cursor or a robotic limb. The goal is to help the person’s own body move again.
This is the strongest example of what people usually imagine when they hear the phrase “restoring movement.” The 2023 Nature paper on a brain-spine interface is important because it showed a wireless digital bridge between the brain and spinal cord that helped a participant regain more natural standing and walking patterns after paralysis. That is a different class of result from simple on-screen control.
2. Spinal cord stimulation systems
These systems do not always require a brain implant. Instead, they target the spinal networks below the lesion. With the right stimulation pattern and enough rehabilitation, these networks can sometimes be pushed back into a state where voluntary intent and sensory feedback become usable again.
This is what made earlier spinal neuromodulation studies so important. They showed that the spinal cord is not always “silent” after injury. In some patients, the circuitry can still respond if it is stimulated in the right way and trained intensively. A helpful comparison is a disconnected orchestra that still knows how to play once timing and coordination are restored.
3. Brain-computer interfaces for digital or robotic control
These systems are different again. Instead of trying to restore native movement directly, they let a person control a computer, communication system, or external device through neural signals. For someone with severe upper-limb paralysis, that may mean typing, clicking, messaging, or operating assistive hardware.
This matters because independence is not only about walking. It is also about communicating, working, controlling the environment, and reducing constant reliance on other people for basic tasks. That is why a company like Synchron matters in this story even though its early human work is more about control than full limb restoration.
What direct movement restoration looks like today
The most meaningful direct movement restoration results still come from spinal stimulation and brain-spine bridging, not from brain chips alone.
The 2018 Nature study on targeted neurotechnology remains foundational because it showed that spatiotemporal epidural stimulation, paired with rehabilitation, could restore stepping and standing functions in people with spinal cord injury. That result mattered not because it instantly cured paralysis, but because it proved that carefully tuned stimulation could engage motor circuits below the injury in a functionally useful way.
The 2023 brain-spine interface study pushed the field further. Instead of relying only on preprogrammed spinal stimulation, it used cortical signals associated with intended lower-limb movement to trigger and modulate spinal stimulation in real time. In plain language, the system listened for intention at the brain level and translated it into stimulation patterns that could support real stepping and standing.
That is a major shift. It turns the technology from a static support system into a dynamic bridge.
Still, this is where realism matters. These achievements do not mean a person with paralysis receives a chip and walks out of the hospital a few days later. They depend on surgical implantation, careful fitting, software calibration, rehabilitation intensity, and continued clinical support. They also come from highly selected cases in expert centers.
Hand and arm restoration remain harder. Lower-limb stepping has received more attention partly because spinal locomotor circuitry can be organized and rhythmically activated in a way that lends itself to stimulation-based support. Fine hand control is more demanding. Yet the March 2026 report about China’s approved brain implant paired with a soft robotic glove is still notable because it points toward a practical middle path: if full biological hand recovery is not yet available, assisted hand function may still be restored in a way that matters day to day.
Where Synchron and other BCIs fit
Synchron’s role in this space is easy to misunderstand if people expect every BCI to restore walking.
The company’s SWITCH study focused on a fully implanted endovascular brain-computer interface for people with severe paralysis. The key difference is the route of implantation. Instead of opening the skull to place electrodes on or in the brain, the device is delivered through blood vessels to a location near motor cortex. That makes the approach less invasive than many traditional implanted BCIs.
What did that system restore? Not over-ground walking or direct arm movement. Its early value was safer implantation and feasible long-term thought-controlled digital switching. For people with severe paralysis, that can mean communication, computer access, and a path toward broader assistive control. That is still a meaningful clinical outcome.
A 2025 follow-up study added something equally important: signal stability over time. In this field, a system is not useful just because it works once in a demo. It has to remain usable across months and ideally years. Long-term signal quality is one of the hidden make-or-break issues in neuroprosthetics.
So where does Synchron fit in the larger landscape?
It fits as part of the autonomy layer. Brain-spine interfaces aim to restore native movement pathways. Systems like Synchron’s Stentrode aim to restore communication and control with lower surgical burden. For many patients, especially those who are not good candidates for complex restorative implants, that may be the more realistic near-term benefit.
This is also why the phrase “medical AI breakthroughs” needs restraint here. AI helps with signal decoding and system responsiveness, but the clinical value still comes from hardware reliability, surgical safety, rehab design, and the patient’s real-world ability to use the system. AI is part of the stack. It is not the whole story.
What families and clinicians should keep in view
The hopeful version of this field is true, but only if it is paired with boundaries.
First, eligibility matters. Not every form of paralysis is the same. A traumatic spinal cord injury, ALS, stroke-related paralysis, and advanced neuromuscular degeneration create very different clinical contexts. A system that helps one subgroup may be irrelevant or unsafe for another.
Second, surgery still matters. Even when a device avoids open-brain surgery, it is not “simple.” These are specialized procedures with follow-up needs, device management, and risk considerations. That is especially important for caregivers who may hear the word “implant” and assume a smooth consumer-style upgrade path. This is still medicine, not consumer electronics.
Third, rehabilitation is not optional. Many of the most exciting results depend on training, calibration, and repeated clinical adjustment. The implant is part of the therapy, not the whole therapy. A useful comparison is a joint replacement: the hardware matters, but outcomes also depend heavily on rehab and patient engagement. Neural restoration systems are even more dependent on that full ecosystem.
Fourth, approval does not mean broad access. A regulatory milestone may signal that a device has crossed a meaningful threshold, but availability can still be limited by cost, geography, clinical infrastructure, and training capacity. A world first approval is not the same as routine availability in community settings.
This is the part that families deserve to hear clearly. The field offers more real hope than it did a few years ago. It still does not offer simple timelines or uniform outcomes.
What this means for the next few years
The next stage of progress is less about proving that restoration is possible and more about making it repeatable.
That means larger clinical studies, better patient selection, lower surgical burden, stronger signal stability, and systems that hold up outside a hero-case environment. It also means combining approaches. A future care pathway may involve spinal stimulation, brain-driven decoding, robotics, and rehabilitation software working together rather than one magic implant doing everything.
Closed-loop control will be central to that shift. The more a system can read intent or biomechanical state and respond in real time, the more natural and useful it becomes. That is why even non-invasive closed-loop spinal stimulation matters in this conversation. It shows that restoration is not only about invasive chips. It is about smarter interfaces between intention, stimulation, and movement.
The likely near-term future is not the end of paralysis in a blanket sense. It is something more concrete and, in some ways, more important: selected patients regaining specific functions that were previously out of reach. For one person, that may be stepping in rehab. For another, it may be controlling a digital interface independently. For another, it may be assisted hand movement that makes feeding or communication easier.
That is how this field usually advances. Not in one cinematic leap, but in layers of restored function that gradually move from extraordinary to expected.


Final Thoughts
Neural implants for paralysis are no longer just a futuristic headline. In 2026, the strongest evidence shows real restoration of movement and control in carefully selected patients. That is a serious medical advance.
But the honest version is better than the dramatic one. The field is not ending paralysis across the board. It is building workable bridges around specific kinds of damage, often with surgery, software, stimulation, and long rehabilitation all working together. For clinicians, caregivers, and readers trying to understand what matters now, that is the right lens: less miracle language, more functional recovery that is finally becoming real.