If you want a clear answer instead of a futuristic sales pitch, here it is. Researchers are building forms of nano-medicine that can target clots, sense narrowed vessels, and deliver drugs more precisely inside blood vessels. But as of April 2, 2026, doctors are not routinely sending autonomous nanobots through the bloodstream to scrub plaque off artery walls. This guide explains what Nanobots in Bloodstream really means, what the best vascular research has already shown, where the science still falls short, and what matters now if your real goal is a longer life with healthier arteries.
What “nanobots in the bloodstream” actually means
The phrase sounds simple, but it hides several very different technologies.
The first group is nanoparticles. These are tiny carriers made from lipids, polymers, metals, or other materials that can transport a drug or imaging agent through the body. They do not move around like miniature submarines. They are closer to highly engineered cargo packages that travel with blood flow and are designed to release or accumulate in the right place.
The second group is DNA nanodevices. These are nanoscale structures built from folded DNA. Some can open, close, or change shape when they sense a trigger such as a clotting signal, a pH shift, or a mechanical force. The best way to picture them is as molecular packages with a lock, a sensor, and a release mechanism.
The third group is microrobots. These systems are still microscopic, but they are closer to what most people imagine when they hear the word robot. They may be guided by magnets, light, ultrasound, or fluid forces, and in some cases they can self-assemble into larger working structures.
This distinction matters because the public conversation often blurs it. Many articles imply that a free-moving cleanup crew is already close to sweeping arteries from the inside. Most of the serious vascular work is less dramatic and more believable. It focuses on targeted delivery, local activation, better clot breakdown, and selective treatment inside a difficult biological environment.
Why arteries become the bottleneck in a 100-year life
If the dream is a healthy 90 or 100 years, artery health matters because cardiovascular disease still dominates the mortality picture. The American Heart Association’s January 21, 2026 statistics update said heart disease remains the leading cause of death in the United States. The same update reported 915,973 U.S. deaths from cardiovascular disease in 2023 and noted that someone died of cardiovascular disease about every 34 seconds.
That is the real reason “artery repair” gets tied to life extension. A longer lifespan depends heavily on keeping blood flowing to the heart, brain, kidneys, and limbs for decades.
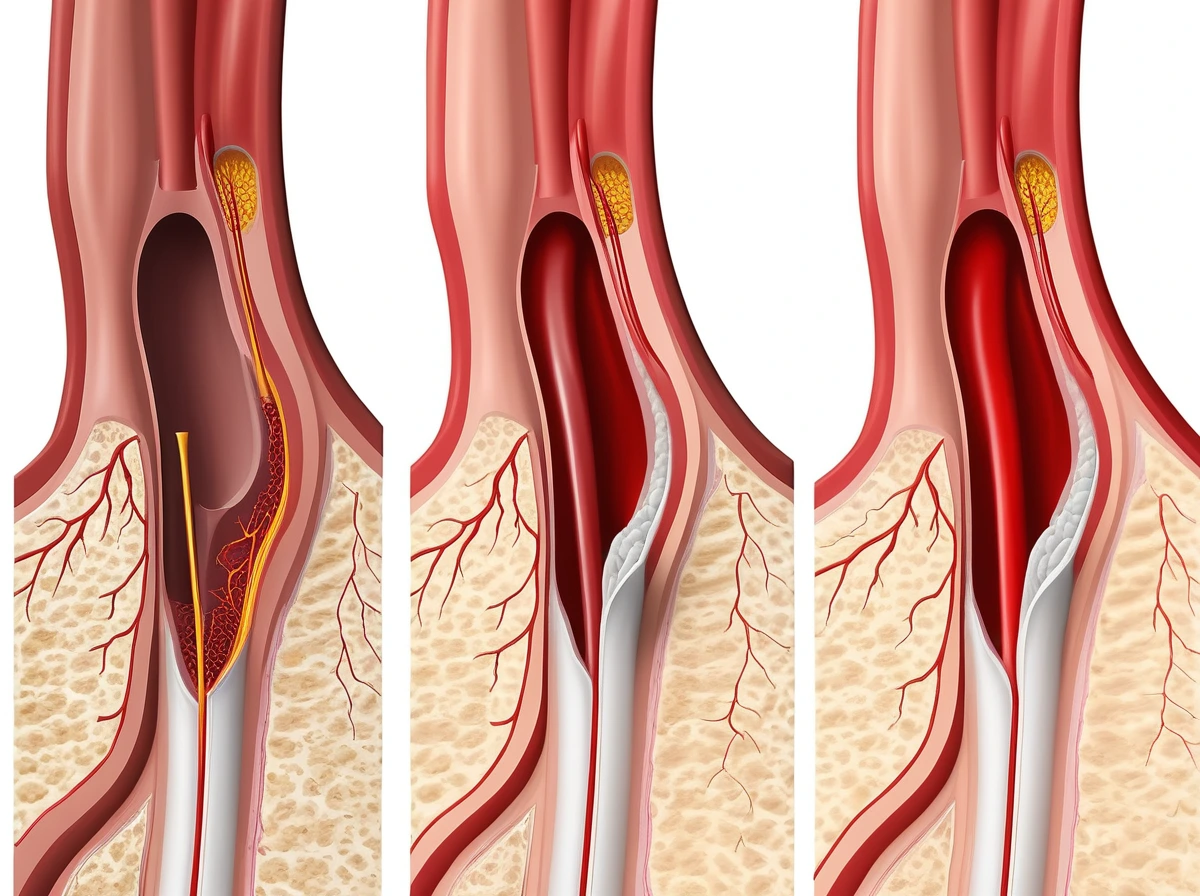
It also helps to separate three related problems that are often mixed together.
Plaque is the long, slow buildup of cholesterol, inflammatory cells, calcium, and scar-like material inside the artery wall. That is atherosclerosis. The American Heart Association’s atherosclerosis explainer describes it as plaque deposits that narrow arteries and make them less flexible.
A clot is different. A clot is a more sudden blockage made from blood components. It can form on top of damaged plaque or elsewhere in the circulation and can obstruct flow quickly.
A narrowed artery, also called a stenotic artery, is the mechanical result. The passage is tight enough to alter blood flow and raise risk.
A simple comparison helps. Plaque is slow structural damage inside the wall. A clot is a sudden blockage that can form on top of a dangerous surface. A narrowed artery is the hemodynamic consequence, meaning the blood now moves through a tighter space with very different forces acting on the vessel and any therapy inside it.
That is why “cleaning arteries” is an awkward but incomplete phrase. Some emerging nano-medicine is aimed at inflammation inside plaque. Some is aimed at dissolving clots. Some is aimed at releasing drugs only where the flow pattern tells the system a vessel is dangerously narrow.
How nano-medicine could help without literally “scrubbing” arteries
The near-term vision is not a tiny janitor with a brush. It is precision therapy inside a crowded and fast-moving highway.
One major target is the inflammatory core of atherosclerotic plaque. A macrophage is an immune cell that engulfs debris. Inside plaque, macrophages can swallow cholesterol and become foam cells, which help drive inflammation and instability. Another key term is efferocytosis, which means clearing dead or dying cells. When that cleanup fails, more debris accumulates and the plaque becomes harder to control.
That is why a lot of nano-medicine work does not aim to grind plaque away mechanically. It aims to change plaque biology. The idea is to deliver a therapy locally, reduce inflammation, improve cleanup, and make the lesion less dangerous.
A concrete example came from a 2024 Nature Communications study in a large-animal model of atherosclerosis. The researchers tested pro-efferocytic nanotherapies in genetically modified pigs and reported reduced vascular inflammation without inducing anemia. That is not the same as instantly erasing years of plaque. It is still important, because it targets a real driver of disease and does so in a model closer to human physiology than the usual mouse-only story.
The broader picture from a 2025 Journal of Translational Medicine review is similar. Atherosclerosis-focused nanotherapeutics are being designed to target macrophages, reduce plaque burden and inflammation, and respond to plaque microenvironments. In other words, the realistic future is targeted biological control, not a mechanical polish of every artery wall.
Where the most advanced work already starts to look futuristic
This field does produce examples that sound like science fiction, and they are worth understanding because they show why the topic keeps attracting attention.
One of the clearest examples is a Nano Letters paper published on January 5, 2026 describing a mechanoresponsive DNA origami capsule for narrowed or obstructed arteries. DNA origami means scientists fold DNA strands into a designed nanoscale shape. In this case, the capsule was built to open under high shear, the physical force created when blood rushes through a tight vessel segment.
That design is clever because it uses the problem itself as the trigger. The capsule stays closed under ordinary flow and opens when pathological flow conditions stretch its DNA spring. It is not a free-swimming robot making independent decisions. It is more like a force-sensitive package that opens when traffic conditions tell it it has reached a dangerous bottleneck.
Another example came from Nature Materials in 2024. Researchers described an intelligent DNA nanodevice for precision thrombolysis. Thrombolysis means dissolving a blood clot. Their system used thrombin-responsive DNA fasteners to help deliver tissue plasminogen activator, or tPA, more precisely. That matters because tPA can save tissue in the right situation, but off-target exposure raises bleeding risk.
This is a good example of where vascular nanotechnology looks especially promising. Clots are more discrete targets than decades-old plaque. Local chemistry can help trigger the right release in the right place. The device is still experimental, but the logic is strong.
Then there is the visibly robotic end of the field. A 2024 Small study indexed in PubMed described a magnetically powered microrobotic swarm for thrombolysis. Under a rotating magnetic field, the particles could self-assemble into longer chain-like structures, penetrate thrombi, and combine mechanical disruption with photothermal and photodynamic treatment. The authors reported about a 90% reduction in thrombus weight in thrombolysis assays.
That is much closer to the popular picture of a miniature cleanup crew. It is also a reminder to stay precise. The target there was thrombus, not mature atherosclerotic plaque embedded in an artery wall for years.
Why this is still experimental medicine
The distance between a striking lab result and routine care is large, especially in cardiology.
The first reason is that human atherosclerosis is slow, messy, and heterogeneous. A plaque in one patient with diabetes, kidney disease, and calcification is not the same as a plaque in a cleaner experimental model. The 2025 translational review is explicit that preclinical success does not guarantee human efficacy.
The second reason is targeting. A nanoparticle or microrobot moving through blood does not encounter a neat cartoon vessel. It encounters proteins, immune cells, branching flow, different vessel sizes, and organs ready to clear foreign material. Even if a platform reaches plaque, it still has to avoid causing trouble elsewhere.
The third reason is safety. Clot-dissolving systems must reduce bleeding rather than shift the danger somewhere else. Plaque-targeting systems must avoid worsening inflammation. Complex coatings, metals, and responsive chemistries all add manufacturing and toxicology questions.
The fourth reason is control. Popular nanobot narratives imply exact navigation through the vascular tree. In reality, control inside tiny, branching, pulsating vessels remains hard. Magnets can help. Flow-sensitive design can help. Molecular triggers can help. But precision in living circulation is still an engineering challenge, not a standard clinical feature.
The fifth reason is scale. A platform has to be manufactured reproducibly, stored reliably, and tested under strict regulatory conditions. That part rarely makes headlines, but it often decides what reaches patients.
So the best summary is straightforward: the science is real, the promise is real, and the clinic is still behind the laboratory.
What matters now if your real goal is longer artery health
For an aging reader, this is the practical bottom line. If the goal is healthy longevity, the tools doing the most work right now are still the proven ones.
The NHLBI’s treatment guidance for atherosclerosis is clear about the present-day baseline. Care focuses on managing cholesterol, blood pressure, blood sugar, smoking exposure, weight, sleep, and physical activity. It also includes medicines such as statins and other cholesterol-lowering therapies, anti-clotting medicines in the right settings, thrombolytics for certain clot-related emergencies, and procedures such as angioplasty and stenting when needed.
That may sound less glamorous than a fleet of nanobots. It is still the part of the story that changes outcomes now. Lower LDL cholesterol, controlled blood pressure, no smoking, better fitness, and timely medical treatment reduce the burden that future nano-medicine is trying to solve more elegantly.
The AHA’s 2026 update points readers toward Life’s Essential 8 for the same reason: eat better, move more, avoid tobacco, sleep well, manage weight, control cholesterol, control blood sugar, and control blood pressure. That is not an anti-technology message. It is the current evidence base.
What should readers watch over the next decade instead of waiting for a miracle?
Watch for more large-animal data. Watch for therapies that release drugs only in diseased vascular environments. Watch for better clot-targeting systems that reduce systemic bleeding risk. Watch for narrow, well-designed early translational studies with clear cardiovascular endpoints.
What not to expect soon is a standard cardiology visit where autonomous nanobots roam every artery and leave it spotless. The nearer-term future is likely to be quieter and more useful: smarter local drug delivery, safer thrombolysis, and better control of plaque biology.
Final Thoughts
The appeal of artery-cleaning nanobots is obvious. If cardiovascular disease is still one of the biggest barriers to a long life, why not send tiny machines in to fix the problem directly?
What the best evidence shows is more grounded and, in some ways, more useful. The future of vascular nano-medicine is likely to be selective, responsive, and biological. It may help drugs reach inflamed plaque more effectively. It may help clot treatment become more precise. It may allow therapies to respond to the force or chemistry of diseased vessels in ways ordinary pills cannot.
That is impressive enough without overstating it. The most accurate answer today is this: nanobots in the bloodstream are becoming a real research tool, but they are not yet cleaning human arteries as a standard therapy. Until that changes, the most effective path to longer artery health is still proven cardiovascular care, with a careful eye on where nano-medicine is genuinely advancing.